
Research Article | DOI: https://doi.org/10.31579/2692-9562/007
Institutional address: Komfo Anokye Teaching Hospital, P.O. Box 1934, Kumasi- Ghana
*Corresponding Author: Anna Konney, Institutional address: Komfo Anokye Teaching Hospital, P.O. Box 1934, Kumasi- Ghana
Citation: Konney A, Dzogbefia M, Philip O Peprah, Gyimah D and Barnor I. (2020) Thyroidectomy under Local Anaesthesia; Experience from a Tertiary Hospital in Kumasi, Ghana. Journal of Clinical Otorhinolaryngology, 2(2): Doi: 10.31579/2692-9562/007
Copyright: © 2020. : Anna Konney, This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
Received: 23 June 2020 | Accepted: 02 July 2020 | Published: 06 July 2020
Keywords: thyroidectomyꓼ regional cervical plexus blockꓼ local anaesthesiaꓼ outcomes
Objectives: Improvement in anaesthesia has allowed thyroidectomies to be performed mainly under general anaesthesia. There is however a growing interest in performing thyroid surgery under local or regional anaesthesia. The objective of this study was to analyse and share our experience with safety of thyroidectomy under regional cervical plexus block/ local anaesthesia in a tertiary referral hospital in Ghana.
Materials and Methods: A retrospective study was conducted on all patients who had thyroidectomy under local anaesthesia from 1st January 2017 to 31st May 2018 in KATH. Data collected were demography, grade of goitre, operating time, and duration of hospital stay, complications and cost effectiveness of the procedure. Data was analysed using Stata version 16.0software.
Results: A total of 105 thyroidectomies were done in the study period out of which 16 were done under local anaesthesia. All 16 patients (16 females, 100%) and majority 11 (68.75%) were aged between 30 and 50 years. 11 (68.75) had grade IB goitres. The most frequently performed surgery was thyroid lobectomy 12 (75%) and in 75% of cases the surgery was completed between 60 and 90 minutes. Most patients, 9 (56.25%) were discharged home within 48 hours following surgery. The cost of treatment was averagely 30% less compared to same surgery under general anaesthesia. No complications were recorded in the post-operative period.
Conclusions: Comprehensive clinical assessment and careful patient selection for thyroidectomy under local anaesthesia result in good surgical outcomes. The procedure is safe and cost-effective and should be performed by experienced surgeons for the best outcomes.
Thyroidectomy is the most common surgery performed for goitre in Ear Nose and Throat (ENT) Department, Komfo Anokye Teaching Hospital (KATH), Ghana due to high referrals from peripheral hospitals in the region and the whole country at large.
Historically, Dunhill T.P. as far back as 1908 described that thyroid surgeries were performed under local anaesthesia for a variety of indications including solitary nodules and toxic goitres [1, 2]. Improvements in anaesthesia has allowed the surgery to be performed mainly under general anaesthesia [3] with local anaesthesia restricted to those patients with contraindications to general anaesthesia [4]. There is however a growing interest in performing thyroid surgery under local or regional anaesthesia [3].
The scope of indications may be widened depending on the experience of the surgeon and anaesthetist. Local anaesthesia may be converted to general at any point in the surgery, and the surgeon and anaesthetist must be prepared to do the conversion [5]. There is no data available on thyroidectomy under local/regional anaesthesia in Ghana.
The aim of this study was to analyse and share our experience with safety of thyroidectomy under regional cervical plexus block/ local anaesthesia at the ENT Department-KATH.
this was a retrospective study conducted in KATH, a tertiary referral hospital in Ghana from 1st January 2017 to 31st May 2018. All patients who had thyroid surgeries under regional cervical block/ local anaesthesia in ENT Department, KATH were included in this study. These patients were euthyroid or were rendered euthyroid prior to surgery. They had no suspicion of malignancy on FNAC and no retrosternal, retro-pharyngeal or retro-tracheal extensions on radiological investigations. All the patients were informed about the possibility of converting to general anaesthesia in case of intolerability of local anaesthesia or other adverse reaction to the drugs. All patients had thorough preoperative counselling and consented for the surgery.
The data collected were demography, grade of goitre, operating time, and duration of hospital stay, complications and cost effectiveness. Patients who had thyroidectomy under general anaesthesia, previous thyroid surgeries, intrathoracic extension, malignancies, huge goitres, and bilateral thyroid involvement were excluded.
All the surgeries were performed by the same surgeon who was comfortable during surgery and was able to identify the recurrent laryngeal nerve and also to communicate with the patient for voice feedback and assessment of the comfort of the patient.
Procedure: The surgeon performed the superficial cervical plexus block in all the patients.
Technique of Superficial Cervical Plexus Block:
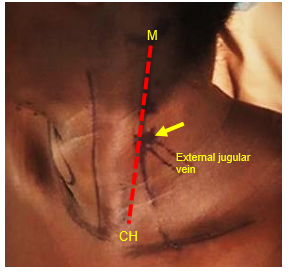
The patient is put in supine position and the head is slightly elevated and extended with the patient’s face turned away from the side that required surgery. (Picture 1)

The anterior and posterior borders and clavicular head of the sternocleidomastoid (SCM) muscle, mastoid tip and clavicle are identified and marked. A vertical line is drawn from the mastoid tip to the clavicular head of the SCM. The crossing point of the external jugular vein (EJV) is identified at the posterior border of the SCM. Most often the Erb’s point is located just above this point (Picture 2).
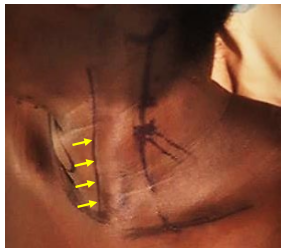
The four branches of the superficial cervical plexus (greater auricular, lesser occipital, transverse cervical, and supraclavicular) emerge at the posterior border of the sternocleidomastoid muscle at Erb’s Point. For local anaesthetic, 1% Lidocaine in 1ꓽ 100 000 adrenaline dilution is used. About 15mls of local anaesthetic is injected at Erb’s point just 1 to 2 cm deep for needle to enter the subplatysmal space (Picture 3).

The needle is advanced along the posterior border of the SCM and posteriorly in a” fan shaped” technique for even distribution of the anaesthetic to block all branches of the superficial cervical plexus (Picture 4).

The anterior border of the SCM is also injected subplatysmal with 10mls of the local anaesthetic to block the terminal anterior branches of the transverse cervical nerve (Picture 5).
The planned collar incision line is infiltrated with 10mls of local anaesthetics before the incision.
Intraoperatively, the patients’ vital signs were monitored by the anaesthetist and they were maintained in a state of mild, conscious sedation with intravenous analgesics (Fentanyl) and mild sedative (Midazolam). No bilateral block was done to avoid transient recurrent laryngeal nerve paralysis and airway compromise. The surgeon was able to monitor the recurrent laryngeal nerve during the procedure.
Statistical Analysis
Data was analysed using Stata version 16.0 software.
Ethical Considerations
The study received ethical approval from the Institutional Review Board (KATH-IRB). Permission was given to collect relevant data from the patients’ folders in total confidentiality.
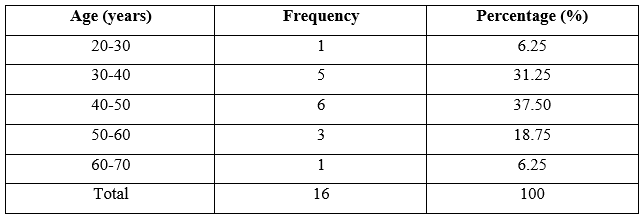
A total of 105 thyroidectomies were done in the study period out of which 16 were done under Superficial Cervical plexus block/ Local anaesthesia. All 16 patients (16 females, 100%) fulfilled the inclusion criteria and were recruited in the study. Majority of the patients 11 (68.75%) were aged between 30 and 50 years. (Table 1).
By the WHO Grade of goitres, majority 11 (68.75) of the thyroidectomies were done for patients who had grade IB goitres and the rest, 5 (31.25%) had grade II. The duration of surgery is represented in (Figure 1).
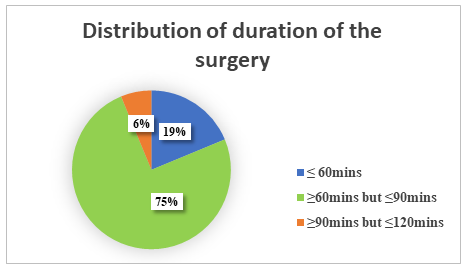
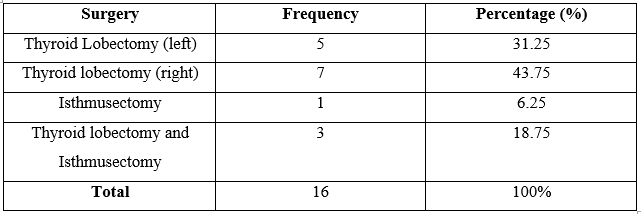
Most of the surgeries were completed between 60 and 90minutes. The most frequently performed surgery was thyroid lobectomy 12 (75%) (Table 2).
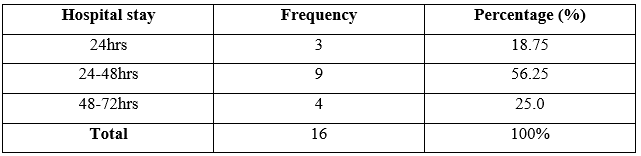
None of the patients stayed more than 72 hours on the ward. Most patients, 9 (56.25%) were discharged home within 48 hours following surgery. Three patients were discharged home 24 hours following surgery (Table 3).
The study revealed a significant association (p-value less than 0.05) between surgery duration and age, type of surgery performed and hospital stayed. Surgery duration was statistically significant with age (X2 =24.0, p =0.002). Also, the type of surgery performed and hospital stay showed a statistically significant association with the surgery duration (X2 =12.44, p =0.042) and (X2 =19.0, p<0>

The bills on discharge of the patients who had the surgery under local anaesthesia were found to be averagely 30% less than those who had the same surgery under general anaesthesia.
No complications were recorded and all the patients were satisfied during the surgery and in the post-operative period. The surgeons were comfortable using this method of anaesthesia.
Prior to the year 2017 all thyroid surgeries in KATH were done under general anaesthesia with intubation.
The selection of suitable patients for thyroidectomy under local anaesthesia is very important. Contraindications to the procedure include large goitres, previous neck surgery, sleep apnoea, coagulopathies, obesity, retro-oesophageal or retro-tracheal goitres, intrathoracic goitres that would require a sternotomy, preoperative recurrent laryngeal nerve paralysis, known or suspected locally invasive cancer and patient’s preference for general anaesthesia.
Coincidentally, our study population of 16 were all females. Aliyu et al [6] had majority (88%) of patients operated under local anaesthesia in Northeastern Nigeria. All our patients cooperated well with the procedure and none was converted to general anaesthesia. Some of the factors that may necessitate conversion from local/regional anaesthesia to general anaesthesia include an unexpected intraoperative pathology, a reaction to the local anaesthetic agent and patient discomfort [7].
Studies have shown that local/regional anaesthesia is safe and effective to be used in surgeries of the thyroid [5, 6, 8, 9, and 10]. A crucial prerequisite for this is the availability of an anesthesiologist or a surgeon who is skilled in the administration of superficial and/or deep cervical blocks and proper levels of sedation [11]. In this study the surgeon successfully performed the local blocks.
The advantages of performing thyroidectomies under local/regional anaesthesia are numerous including the reduction in the risks associated with general anaesthesia such as the risks associated with endotracheal intubation and the untoward effects of anaesthetic agents [10, 12]. This is of particular benefit to singers and public speakers as studies have shown that endotracheal intubation is associated with vocal cord changes in about 5% of patients [8]. Again, both patients and surgeons alike find the avoidance of minor side effects like nausea, vomiting, headaches, drowsiness, pharyngitis and visual problems attractive [5].
Recovery from anaesthesia is also faster, when compared to general anaesthesia. Only 3 out of 16 patients were discharged within 24 hours after surgery. This contrasts with the study describing experience with outpatient thyroidectomy [13], where 76 out of 134 patients were discharged the same day after a postoperative evaluation period of 4 to 8 hours.
Overall cost of treatment for patients undergoing thyroidectomy under local/regional anaesthesia is lower than patients who had thyroidectomy under general anaesthesia as demonstrated in our study and also in Brazil [9, 10, and 14]. Ultimately, local/regional anaesthesia has been found to be superior in patients with compromised cardiac status and those with symptoms of obstruction due to a large goitre to avoid the risks associated with a difficult intubation [11, 15].
Major complications associated with LA/regional anaesthesia may include accidental injection into the internal jugular vein or carotid artery, direct infusion into the thyroid veins resulting in local anaesthetic toxicity and infiltration of the vagus nerve resulting in transient vocal cord paralysis and potential airway loss, resulting in the need for conversion to general anaesthesia.
Comprehensive clinical assessment and careful patient selection for thyroidectomy under local anaesthesia/superficial cervical plexus block result in good surgical outcomes, and these can be replicated successfully with great care in low resource settings where there is lack of anaesthetic services for endotracheal intubations. Such thyroidectomies are tolerable and also cost-effective and should be performed by experienced surgeons for the best outcomes.
Dear Editorial Team, Clinical Medical Reviews and Reports. My experience with the journal was highly positive. The peer-review process was rigorous, constructive, and completed in a timely manner. The reviewers provided valuable comments that helped improve the quality and clarity of our manuscript. The editorial office was professional, responsive, and supportive throughout all stages of the publication process. Communication was clear and efficient, and any questions were addressed promptly. Overall, I found the journal to maintain high scientific standards and an excellent publication workflow. I would be pleased to consider submitting future work to this journal. Best wishes from, Elena Popa.

It was my pleasure to submit my testimonial concerning the Reviewer Board of our Scientific Journal “Brain and Neurological Disorders”. The Reviewers focused on some modifications and their contribution was helpful. The ladies of our Editorial Office were also supported my efforts. It was my honor to have such a co-operation and I am looking forward for more collaboration.

Dear Grace Pierce, Editorial Coordinator of Journal of Clinical Research and Reports, Thank you for the speedy and efficient peer review process. I appreciate the fact that your peer reviewers do not take months to respond like with some other journals. I would also like to thank the editorial office for responding quickly to my questions. It is an excellent journal. I plan to submit more manuscripts in the future. Best wishes from, Robert W. McGee

Dear Grace Pierce, Editorial Coordinator of Journal of Clinical Research and Reports, Working with you and your team on our recent publication in JCRR has been a truly wonderful and enjoyable experience. The responses were prompt, and the reviewers were patient, constructive, and highly professional. One reviewer in particular gave me the feeling that a professor was carefully reading and commenting on my coursework, which was deeply touching. The entire process was straightforward and hassle‑free, with no tedious online forms to complete. I highly recommend this journal. Best wishes from, DR Aibing Rao, Head of R&D

I Appreciate the Opportunity to Share my Experience with the Journal of Clinical Research and Reports. The peer review process was timely and constructive, and the feedback provided helped improve the quality of our manuscript. The editorial office was professional, responsive, and supportive throughout the process, ensuring smooth communication and efficient handling of the submission. Overall, it was a positive experience collaborating with your team.

Dear Mercy Grace, Editorial Coordinator of Obstetrics Gynecology and Reproductive Sciences, We would like to express our gratitude for your help at all stages of publishing and editing the article. The editors of the magazine answer all the necessary questions and help at every stage. We will definitely continue to cooperate and publish other works in the Obstetrics Gynecology and Reproductive Sciences! Best wishes from, Alla Konstantinovna Politova,
